Understanding SLAP Tears
SLAP tears are common in athletes or individuals who frequently perform overhead motions, such as throwing, swimming, or swinging tools.
They can result in pain, instability, and loss of shoulder function, and represent about 8% of all shoulder injuries.
What is a SLAP tear?
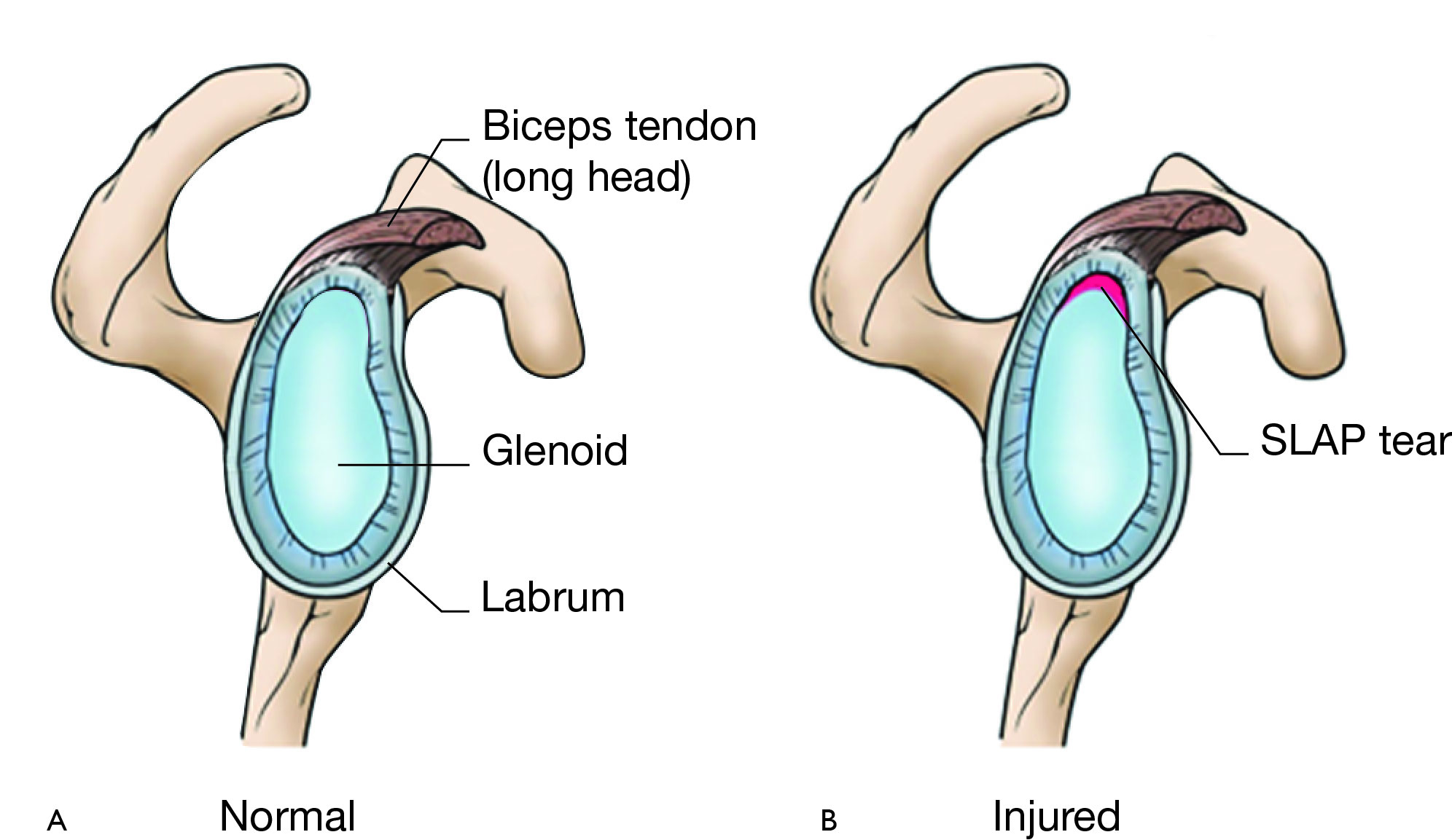
SLAP stands for ‘Superior Labrum Anterior to Posterior’. The term describes a tear in the top part of the labrum, the cartilage that lines the socket of the shoulder joint (called the glenoid).
The labrum helps stabilize the shoulder by providing a secure fit for the head of the upper arm bone (humerus) within the socket.

SLAP tears are typically classified into four basic types:
- Type I (a): Fraying of the labrum with an intact biceps anchor
- Type II (b): The most common (41%), involving a detached biceps anchor and labrum, often seen in throwing athletes. These tears are usually located at the posterior and superior parts of the labrum
- Type III (c): A “bucket handle” tear of the labrum with the biceps anchor intact
- Type IV (d): A “bucket handle” tear extending into the biceps tendon
— Learn more about the basics of labral tears —
What causes a SLAP tear?
Common causes of SLAP tears include:
- Chronic overuse that involves repetitive overhead activities, commonly seen in throwing athletes or those doing repetitive heavy lifting
- Acute trauma including falling on an outstretched arm, a direct impact/blow, a sudden forceful pull like trying to catch a heavy object or lifting something too heavy suddenly, shoulder dislocation
- Degeneration where the labrum wears down with age, making tears more common in those over 40

What are symptoms of a SLAP tear?
SLAP tears can cause a variety of symptoms that include:
- Feelings of locking, popping, catching, or grinding
- Feelings of ‘giving way’, especially with overhead activities
- Pain with movement or holding the shoulder is specific positions
- Pain with lifting, especially overhead
- Persistent ‘deep’ shoulder pain
- Loss of strength
- Throwing athletes may experience a gradual loss of throwing speed or control
How is a SLAP tear diagnosed?
Diagnosing a SLAP tear requires:
- A detailed medical history including symptoms, activities, and prior injuries
- A thorough physical examination of the neck and shoulders to check for trauma, differences in range of motion, strength deficits, and shoulder stability
- Special physical tests such as the O’Brien’s Test or Crank Test
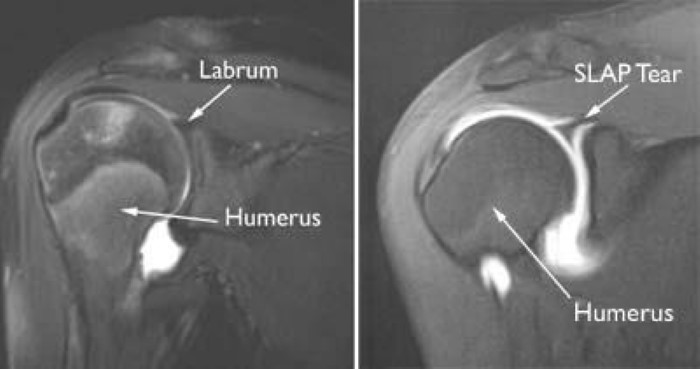
- Imaging, usually involving X-Ray to rule out other reasons for shoulder pain (fractures, bony abnormalities) and MRI of the soft tissues, particularly an MR Arthrogram (MRA) where dye is injected into the joint prior to scanning
How is a SLAP tear treated?
Treatment options depend on the severity of the tear, as well as the patient’s activity level and personal goals.
Non-Operative Treatment
Non-operative treatment is often the first step, especially for mild to moderate tears, or for individuals not participating in high-demand sports / activities. Treatment includes:
- Rest and activity modification to avoid activities that aggravate symptoms.
- Physical therapy for stretching and strengthening to rotator cuff and shoulder stabilizing muscles. Goals of physical therapy include restoring muscle strength, endurance, neuromuscular control, and normal joint movement.
- Medications such as non-steroidal anti-inflammatory drugs (NSAIDs) to reduce pain and inflammation.
- Injection-based therapies may be used when pain persists despite activity modification and NSAIDs. Examples include corticosteroids, platelet rich plasma, and stem cells. However, there is limited data to support these interventions.
Surgical Treatment
Surgery may be considered as an option for patients that don’t show improvement after 3 – 6 months of physical therapy, especially if they’re still experiencing pain, and haven’t been able to regain rotator cuff strength, or return to their previous level of activity.
The two most common surgical options include:
- Arthroscopic Repair – best suited for younger athletes (<30 years old) and high level athletes involved in overhead sports e.g. baseball, tennis, volleyball. This is a minimally invasive, keyhole surgery that involves reattaching the labrum back to the glenoid using knotless anchor repair techniques.
- Biceps Tenodesis – traditionally used for middle-aged individuals (>30 years old), non-overhead athletes, patients with concomitant rotator cuff tears, or those receiving workers’ compensation. It is also the preferred option after failed SLAP repairs. During this surgery, the biceps tendon is detached from the labrum and reattached to the upper arm bone (the humerus).
Post-Surgical Rehabilitation
Postoperative rehabilitation is customized based on the severity of the injury, the extent of the surgical repair, and the patient’s desired functional outcomes.
- Early postoperative phase – specific ROM limits are recommended to minimize stress on the repair while it heals.
- As healing progresses, the focus shifts to strengthening and stabilizing the glenohumeral and scapulothoracic joints.
- Later stages – emphasis moves toward restoring pre-injury strength, conditioning, and functional performance.
- Transition to maintenance phase – this includes a structured return-to-play program designed to support long-term recovery and performance.
Outcomes & Returning to Activities
Most patients improve significantly with proper treatment.
Non-surgical options are often enough for individuals with less demanding shoulder activities.
For athletes, a full return to sports is possible after recovery, but outcomes depend on the severity of the injury and strict adherence to rehabilitation. For example, studies indicate that 40% of professional baseball players are able to successfully return to play through rehabilitation alone, without the need for surgery. Surgery offers a high success rate for pain relief (90%), but returning to elite-level competition is less predictable, with success rates ranging from 22-64%. Postoperative rehabilitation is critical for achieving the best outcomes.
Overall, SLAP tears can be effectively managed with a combination of non-operative and surgical treatments tailored to your specific needs. Understanding your condition and treatment options is essential for making informed decisions about your care.
Contributing Expert
Brandon Spink, Family Medicine PGY3, University of Alberta
References
- Burkhart SS, Morgan CD. The peel-back mechanism: its role in producing and extending posterior type II SLAP lesions and its effect on SLAP repair rehabilitation. Arthrosc J Arthrosc Relat Surg Off Publ Arthrosc Assoc N Am Int Arthrosc Assoc. 1998;14(6):637-640. doi:10.1016/s0749-8063(98)70065-9
- Patiño JM. Superior labral anterior and posterior (SLAP) lesions of the long bicep insertion on the glenoid: management in athletes. Int Orthop. 2022;46(6):1351-1360. doi:10.1007/s00264-022-05385-2
- SLAP Tears in the Shoulder – OrthoInfo – AAOS. Accessed December 24, 2024. https://www.orthoinfo.org/en/diseases–conditions/slap-tears/
- Snyder SJ, Karzel RP, Del Pizzo W, Ferkel RD, Friedman MJ. SLAP lesions of the shoulder. Arthrosc J Arthrosc Relat Surg Off Publ Arthrosc Assoc N Am Int Arthrosc Assoc. 1990;6(4):274-279. doi:10.1016/0749-8063(90)90056-j
- Huri G, Hyun YS, Karahan M, McFarland EG. Superior Labrum Anterior and Posterior Lesions: Evaluation and Treatment. In: Doral MN, Karlsson J, eds. Sports Injuries: Prevention, Diagnosis, Treatment and Rehabilitation. Springer; 2015:365-382. doi:10.1007/978-3-642-36569-0_20
- Powell SE, Nord KD, Ryu RKN. The Diagnosis, Classification, and Treatment of SLAP Lesions. Oper Tech Sports Med. 2012;20(1):46-56. doi:10.1053/j.otsm.2012.03.006
- Digiovine NM, Jobe FW, Pink M, Perry J. An electromyographic analysis of the upper extremity in pitching. J Shoulder Elbow Surg. 1992;1(1):15-25. doi:10.1016/S1058-2746(09)80011-6
- Andrews JR, Carson WG, Mcleod WD. Glenoid labrum tears related to the long head of the biceps. Am J Sports Med. 1985;13(5):337-341. doi:10.1177/036354658501300508
- Varacallo M, Tapscott DC, Mair SD. Superior Labrum Anterior Posterior Lesions. In: StatPearls. StatPearls Publishing; 2024. Accessed December 23, 2024. http://www.ncbi.nlm.nih.gov/books/NBK538284/
- Rokito SE, Myers KR, Ryu RKN. SLAP Lesions in the Overhead Athlete. Sports Med Arthrosc Rev. 2014;22(2):110. doi:10.1097/JSA.0000000000000018
- Tennent TD, Beach WR, Meyers JF. A Review of the Special Tests Associated with Shoulder Examination: Part II: Laxity, Instability, and Superior Labral Anterior and Posterior (SLAP) Lesions. Am J Sports Med. 2003;31(2):301-307. doi:10.1177/03635465030310022601
- Kim SH, Ha KI, Ahn JH, Kim SH, Choi HJ. Biceps load test II: A clinical test for SLAP lesions of the shoulder. Arthrosc J Arthrosc Relat Surg Off Publ Arthrosc Assoc N Am Int Arthrosc Assoc. 2001;17(2):160-164. doi:10.1053/jars.2001.20665
- Cook C, Beaty S, Kissenberth MJ, Siffri P, Pill SG, Hawkins RJ. Diagnostic accuracy of five orthopedic clinical tests for diagnosis of superior labrum anterior posterior (SLAP) lesions. J Shoulder Elbow Surg. 2012;21(1):13-22. doi:10.1016/j.jse.2011.07.012
- Warth RJ, Millett PJ. Disorders of the Long Head of the Biceps Tendon. In: Warth RJ, Millett PJ, eds. Physical Examination of the Shoulder: An Evidence-Based Approach. Springer; 2015:109-138. doi:10.1007/978-1-4939-2593-3_5
- Clark RC, Chandler CC, Fuqua AC, Glymph KN, Lambert GC, Rigney KJ. Use of Clinical Test Clusters Versus Advanced Imaging Studies in the Management of Patients with a Suspected Slap Tear. Int J Sports Phys Ther. 2019;14(3):345-352. doi:10.26603/ijspt20190345
- Jee WH, McCauley TR, Katz LD, Matheny JM, Ruwe PA, Daigneault JP. Superior labral anterior posterior (SLAP) lesions of the glenoid labrum: reliability and accuracy of MR arthrography for diagnosis. Radiology. 2001;218(1):127-132. doi:10.1148/radiology.218.1.r01ja44127
- Jonas SC, Walton MJ, Sarangi PP. Is MRA an unnecessary expense in the management of a clinically unstable shoulder? Acta Orthop. 2012;83(3):267-270. doi:10.3109/17453674.2012.672090
- Sudah SY, Menendez ME, Garrigues GE. Nonoperative Treatment of the Biceps-Labral Complex. Phys Med Rehabil Clin N Am. 2023;34(2):365-375. doi:10.1016/j.pmr.2022.12.004
- Nho SJ, Strauss EJ, Lenart BA, et al. Long head of the biceps tendinopathy: diagnosis and management. J Am Acad Orthop Surg. 2010;18(11):645-656. doi:10.5435/00124635-201011000-00002
- Finnoff JT, Fowler SP, Lai JK, et al. Treatment of Chronic Tendinopathy with Ultrasound-Guided Needle Tenotomy and Platelet-Rich Plasma Injection. PM&R. 2011;3(10):900-911. doi:10.1016/j.pmrj.2011.05.015
- Mautner K, Blazuk J. Where Do Injectable Stem Cell Treatments Apply in Treatment of Muscle, Tendon, and Ligament Injuries? PM&R. 2015;7(4, Supplement):S33-S40. doi:10.1016/j.pmrj.2014.12.012
- Michener LA, Abrams JS, Bliven KCH, et al. National Athletic Trainers’ Association Position Statement: Evaluation, Management, and Outcomes of and Return-to- Play Criteria for Overhead Athletes With Superior Labral Anterior-Posterior Injuries. J Athl Train. 2018;53(3):209-229. doi:10.4085/1062-6050-59-16
- Edwards SL, Lee JA, Bell JE, et al. Nonoperative Treatment of Superior Labrum Anterior Posterior Tears: Improvements in Pain, Function, and Quality of Life. Am J Sports Med. 2010;38(7):1456-1461. doi:10.1177/0363546510370937
- Fedoriw WW, Ramkumar P, McCulloch PC, Lintner DM. Return to Play After Treatment of Superior Labral Tears in Professional Baseball Players. Am J Sports Med. 2014;42(5):1155-1160. doi:10.1177/0363546514528096
- Fortier LM, Menendez ME, Kerzner B, Verma N, Verma NN. SLAP Tears: Treatment Algorithm. Arthrosc J Arthrosc Relat Surg. 2022;38(12):3103-3105. doi:10.1016/j.arthro.2022.08.005
- Althoff AD, Brunette C, Brockmeier S. Postoperative Rehabilitation After Superior Labrum Anterior Posterior Repair. Phys Med Rehabil Clin N Am. 2023;34(2):377-392. doi:10.1016/j.pmr.2022.12.005