
Return to Sport after ACL injury: ACL experts develop a consensus
“When can I return to sport?” is a common question asked by patients following anterior cruciate ligament (ACL) injury.
The answer to this question is complex and dependent on a variety of injury and patient factors.
To clarify the definition and criteria surrounding return to sport (RTS), 26 international ACL experts got together to develop several consensus statements that were recently published by Meredith and colleagues in the Knee Surgery, Sports Traumatology, Arthroscopy journal (1).
Key Points of the Consensus Paper
- RTS is defined as achieving the pre-injury level of sport
- RTS involves a continuum of criteria-based progression from return to participation, to return to sport, and ultimately a return to performance
- RTS decision-making based only on timing should be abandoned
- Decisions on progression along the RTS continuum should be made by a multidisciplinary team involving the patient, caregiver/guardian if the patient is under 18 years of age, surgeon, team physician, and physical therapist/athletic trainer
- Progression along the RTS continuum should incorporate objective physical examination, validated peer-reviewed RTS tests that include functional assessment as well as psychological readiness
- RTS should also consider biological healing of the graft, contextual factors (e.g. type of sport, time of season, position, level of competition, etc), and associated injuries
Read more about the biological healing of ACL grafts
When does the return to sport process start?
The return to sport process starts immediately after ACL injury with a rehabilitation program focused on neuromuscular control, proprioception, and strengthening.
Learn about the Banff Sport Medicine ACL Reconstruction Rehabilitation Program
Initial medical clearance to return to participation/training is given by the physician in collaboration with the treating physiotherapist. This decision is based upon biologic factors, associated injuries, performance on functional testing assessments, and psychological readiness.
Once a patient has been cleared to begin unrestricted training, they can then move through the three phases of the RTS Continuum:
Return to Participation > Return to Sport > Return to Performance
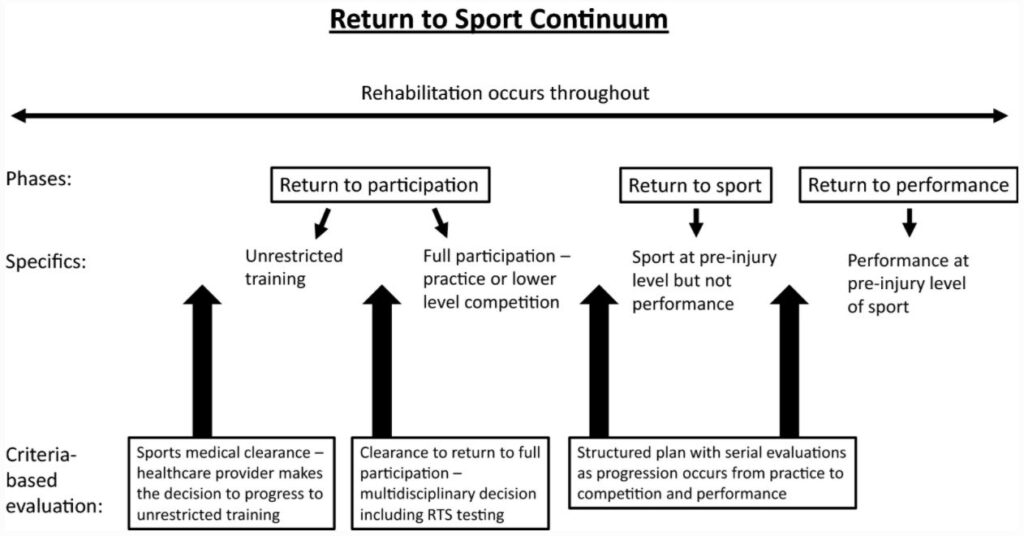
During the phase of return to participation, the patient is physically active, may train, but is medically, physically and/or psychologically not yet ready to return to sport.
During the return to sport phase, the patient has returned to their defined sport, but the desired performance level hasn’t been reached.
During the return to performance phase, the patient has returned to their defined sport and performs at their pre-injury level.

Is timing an important factor when considering a return to sport?
Timing is just one important factor to consider.
Individual differences in biological healing, neuromuscular control, functional skills, and psychological readiness are additional factors.
Research has shown that some of these factors, such as neuromuscular control, and the development of sufficient proprioception and strength after ACL injury could take up to 2 years to regain.
Biological healing and maturation of a graft when ACL reconstruction is the treatment of choice, is another important factor to consider. There is likely a minimum time necessary to allow graft maturation, and RTS prior to 6 months represents an unacceptably high risk of re-injury.
In addition, research studies have shown that for every month RTS was delayed until 9 months after surgery, the reinjury risk was reduced by 51%(2).
Based on the combination of these factors, Meredith and colleagues agreed that RTS criteria based only on timing should be abandoned in clinical practice.
Future considerations
While Meredith and colleagues have provided a clear definition of RTS and proposed some guidelines for the process, they also identified key areas still requiring further research. These include:
- Psychological factors. Psychological readiness to return to sport is clearly an important factor, however, there is currently no clear way to assess it.
- Concomitant (associated) injuries or injuries that occur at the same time as ACL injury are common and can affect timing of RTS. There is, however, a lack of research to guide health care providers and clinicians on how the RTS process should be modified to account for these additional injuries.

Contributing Expert

Dr Michaela Kopka, Orthopaedic Surgeon
References
1.Meredith SJ, Rauer T, Chmielewski TL, et al. Return to sport after anterior cruciate ligament injury: Panther Symposium ACL Injury Return to Sport Consensus Group. Knee Surg Sports Traumatol Arthrosc. 2020;28(8):2403-2414. doi:10.1007/s00167-020-06009-1
2.Grindem H, Snyder-Mackler L, Moksnes H, Engebretsen L, Risberg M., Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: the Delaware-Oslo ACL cohort study. British Journal of Sports Medicine50, 804 (2016).





