
Meniscal ramp lesions: The basics
A meniscal ramp lesion is a type of injury to a specific structure of the medial meniscus called the posterior horn. This is an area of the meniscus at the back of the knee close to where it attaches to the tibia (shin bone).
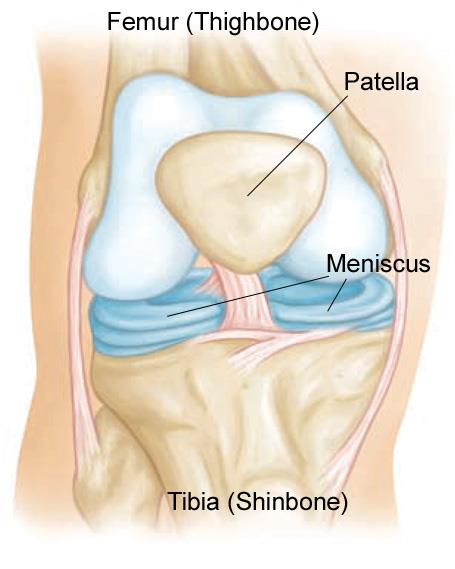
Meniscus – c-shaped pad of cartilage in the knee that acts as a shock absorber.
Ramp lesions are traumatic injuries often associated with ACL injury that are present in up to 40% of ACL tears. They result in a tear or detachment of the posterior horn from the surrounding structures.
Overview of the knee
Location of the posterior horn

Example of a ramp lesion

There is also some research evidence that suggests ramp lesions are more likely to occur in males, patients under 30 years old, patients with complete ACL tears, and when there is an additional lateral meniscal tear.
Why are ramp lesions important?
In addition to distributing load, the medial meniscus contributes to stability of the knee.
Research has shown that the knee is more unstable when there is a ramp lesion with an ACL tear compared to only an ACL tear. In some cases, if the ramp lesion is left unrepaired during ACL reconstruction, it can lead to the failure of the ACL graft.
Ramp lesions also tend to result in pain, particularly around the inner/back or back of the knee when this area of the meniscus is loaded. For example, this pain can occur with deep flexion such as when squatting or kneeling, or with loaded twisting on a flexed knee.
Diagnosis of a ramp lesion
Diagnosing a meniscal ramp lesion primarily relies on a combination of physical examination, history, imaging (MRI), and arthroscopic assessment. Your doctor will ask about how the injury happened (e.g. was it from a twisting or hyperextension motion), where is the pain located, and any other symptoms like locking, popping, or catching of the knee. They will also carrying out a physical exam of the knee, checking for areas of tenderness where the meniscus is location, and carrying out special tests like the McMurray Test that tests for meniscal tears.
While an MRI can be used to diagnose a ramp lesion, it is not as sensitive or specific as arthroscopy (minimally invasive surgery looking into the knee with cameras). This means that a ramp lesion may be diagnosed only at the time of surgery even if an MRI was carried out beforehand.
Treatment of a ramp lesion

If a ramp lesion is identified while examining the posterior horn of the medial meniscus during arthroscopy, the surgeon will make the decision to repair it or not.
Stable ramp lesions, defined as those smaller than 1 cm, do not need specific treatment. Limited research shows there are no differences in outcomes for repair versus conservative management of stable ramp lesions.
If the ramp lesion is unstable or larger than 1 cm, it is repaired with sutures. Research shows good outcomes in patient reported knee function following ACL reconstruction with ramp lesion repair.
Recovery
As ramp lesions are usually repaired at the same time as ACL reconstruction, the post-operative rehabilitation is guided by the post-operative ACL protocol with the following modifications: no kneeling, lunges or squatting beyond 90 degrees for 12 weeks after surgery.
Overall, as this is a relatively new area of research, the understanding of the clinical importance and long-term outcomes of ramp lesions continues to develop. More studies, including long-term follow-up of patients is needed to better guide the diagnosis and management of these types of injuries.
Contributing Expert
Helen Crofts, BSc, MDPGY4 Orthopaedic Surgery, University of British Columbia
References
Bae, B.S., Yoo, S. & Lee, S.H. Ramp lesion in anterior cruciate ligament injury: a review of the anatomy, biomechanics, epidemiology, and diagnosis. Knee Surg & Relat Res 35, 23 (2023). https://doi.org/10.1186/s43019-023-00197-z
Chahla J, Dean CS, Moatshe G, Mitchell JJ, Cram TR, Yacuzzi C, LaPrade RF. Meniscal Ramp Lesions: Anatomy, Incidence, Diagnosis, and Treatment. Orthop J Sports Med. 2016 Jul 26;4(7):2325967116657815. doi: 10.1177/2325967116657815. PMID: 27504467; PMCID: PMC4963625.
Kunze KN, Wright-Chisem J, Polce EM, DePhillipo NN, LaPrade RF, Chahla J. Risk Factors for Ramp Lesions of the Medial Meniscus: A Systematic Review and Meta-analysis. The American Journal of Sports Medicine. 2021;49(13):3749-3757. doi:10.1177/0363546520986817
Marin F, Soto J, Barahona M, Negrin R. Searching for the Best Treatment for Ramp Lesions: A Systematic Review and Network Meta-Analysis. Cureus. 2023 Jul 10;15(7):e41651. doi: 10.7759/cureus.41651. PMID: 37435014; PMCID: PMC10332486.
Rodriguez AN, LaPrade RF, Geeslin AG. Combined Meniscus Repair and Anterior Cruciate Ligament Reconstruction. Arthroscopy. 2022 Mar;38(3):670-672. doi: 10.1016/j.arthro.2022.01.003. PMID: 35248223.
Siboni R, Pioger C, Jacquet C, Mouton C, Seil R. Ramp Lesions of the Medial Meniscus. Curr Rev Musculoskelet Med. 2023 May;16(5):173-181. doi: 10.1007/s12178-023-09834-2. Epub 2023 Apr 4. PMID: 37014609; PMCID: PMC10188848.
Qalib YO, Tang Y, Wang D, Xing B, Xu X, Lu H. Ramp lesion of the medial meniscus. EFORT Open Rev. 2021 May 4;6(5):372-379. doi: 10.1302/2058-5241.6.200126. PMID: 34150331; PMCID: PMC8183152.





