
High Tibial Osteotomy
A High Tibial Osteotomy (HTO) is a type of ‘joint preservation’ surgery that involves cutting the shin bone (tibia) to change the alignment of the knee. It is used to improve symptoms of osteoarthritis by offloading weight from arthritic cartilage inside the knee with the aim of preventing a future knee replacement surgery. In some cases, an HTO can also be used to treat knee instability.
Osteotomy literally means “cutting of the bone”.
Knee osteoarthritis can be simply explained as the degeneration of the smooth bony (articular) cartilage that covers the end of the thigh-bone (femur) as well as the top of the shin bone (tibia). Normally this bony cartilage is smooth and shiny, but with osteoarthritis, it can become thin or develop holes. Patients with osteoarthritis often complain of pain, swelling, and knee stiffness, especially with activity.
Cartilage = the main type of connective tissue throughout your body. In the knee, it acts as a protective cushion between your leg bones as well as with your kneecap (patella).
— To learn more about knee osteoarthritis here —
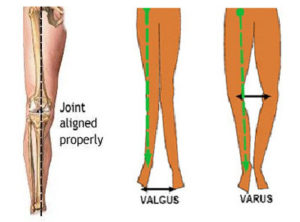
There are three compartments of the knee joint that can develop osteoarthritis; the inner (medial) side, the outer (lateral) side, and underneath the kneecap (patella). Osteoarthritis can sometimes lead to bow-legged (varus) or knock-kneed (valgus) alignment of the knees, depending on which compartment of the knee is affected.
The most common use of HTO is for bow-legged (varus) deformities to offload weight from the arthritic inner medial side of the knee.
In Figure 1 below, the shin bone has been cut at an angle to change its alignment. The bone is then fixed with a plate to allow it to heal in the new position.

Who is the ideal patient to receive an HTO?

An HTO is not recommended for all patients with knee osteoarthritis.
Research shows that HTO is the most effective in people between 40 to 60 years old who are moderately active or have physically demanding work, aren’t overweight, and have osteoarthritis in only one compartment (typically the inner medial knee compartment).
These patients have the greatest likelihood of experiencing pain relief and delaying the progression of knee arthritis and need for a future knee replacement surgery.
What happens during surgery?
Several techniques exist, which involve opening the skin around the knee and cutting the upper shin (tibia) bone.
The two main techniques are “medial opening wedge osteotomy” and “lateral closing wedge osteotomy”. During the osteotomy operation, knee arthroscopy may also be performed to look inside the knee with a tiny camera and assess knee structures.
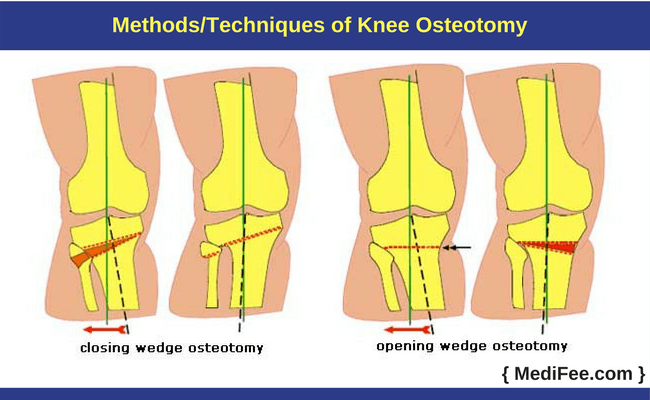
In a lateral closing wedge osteotomy, a wedge is cut in the shin bone (tibia), which is pushed closed, then stabilized with a metal plate and screws.
In a medial opening wedge osteotomy, a cut is made into the shin bone, and it is wedged open. Sometimes the wedge space is filled with a bone graft that either comes from your own pelvis (autograft) or a bone bank (donor allograft) to promote bone healing. This opening in the bone is then stabilized with a metal plate and screws.
Recovery from an HTO
Most patients will stay in the hospital for 1-2 days after surgery.
After going home, your surgeon may prescribe a hinged knee brace for the first 6-12 weeks. After that, the use of a brace and how much weight you’re allowed to place on your leg will depend on the size of your osteotomy and the type of plate the surgeon used for your surgery.
Rehabilitation follows a phased approach, with patients often returning to higher intensity activities 6 months after surgery, depending on your surgeon’s recommendations.
— Learn more about what’s involved in rehabilitation after HTO surgery here —
Outcomes following an HTO
HTO is highly successful in suitable patients and effectively reduces pain and improves knee function in patients with inner compartment (medial) knee osteoarthritis.
Research shows the majority (more than 80%) of patients can return to work or sport by 1 year after surgery.
Contributing Expert

Jenny He, MD Candidate, Faculty of Medicine & Dentistry, University of Alberta
References
Khakha, R. S., Bin A.R., Hamid R., Kley, K., van Heerwaarden, R., & Wilson, A. J. (2021). Role of high tibial osteotomy in medial compartment osteoarthritis of the knee: Indications, surgical technique and outcomes. Journal of Clinical Orthopaedics and Trauma, 23, 101618.
Wright, J.M., Crockett, H.C., Slawski, D.P., Madsen, M.W., Windsor, R.E. (2005). High Tibial Osteotomy. Journal of the American Academy of Orthopaedic Surgeons, 13(4), p 279-289.
Capella, M., Gennari, E., Dolfin, M., Saccia, F. (2017). Indications and results of high tibial osteotomy. Annals of Joint, 2(6):33





