Labral tears of the shoulder: The basics

The shoulder labrum is a fibrous piece of cartilage that resembles a donut and is located between the ball (humeral head) and socket (glenoid) of the shoulder (glenohumeral) joint. It is distinct from the cartilage at the ends of bones (articular cartilage) that enable joints to glide smoothly.
What is the function of the labrum?
The shoulder is not exactly a true ball-and-socket joint. Instead, it resembles a ball resting on a dinner plate, making it inherently unstable. While this structure allows the shoulder to achieve nearly 360° of range of motion, it comes at the cost of reduced stability.
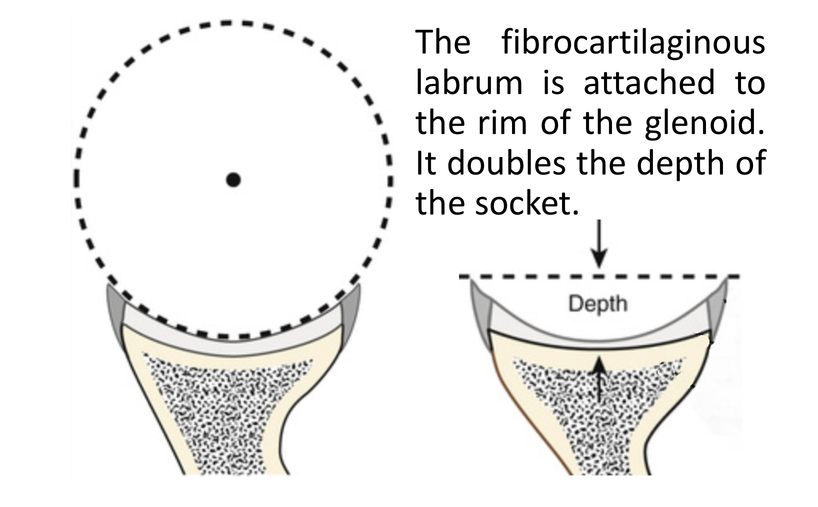
The labrum functions as a cartilaginous ring that deepens the socket, increasing stability by up to 50%. Think of how a golf ball stays on a tee due to the tee’s circular rim, which increases the contact surface with the ball.
Additionally, the labrum serves as an attachment point for other structures that help hold the joint together, such as ligaments and tendons. One example is the biceps tendon. These anchor points are especially important for throwing and overhead athletes, such as volleyball players, pitchers, and swimmers.
What are labral tears and what causes them?
There are several types of labral tears.
SLAP tears
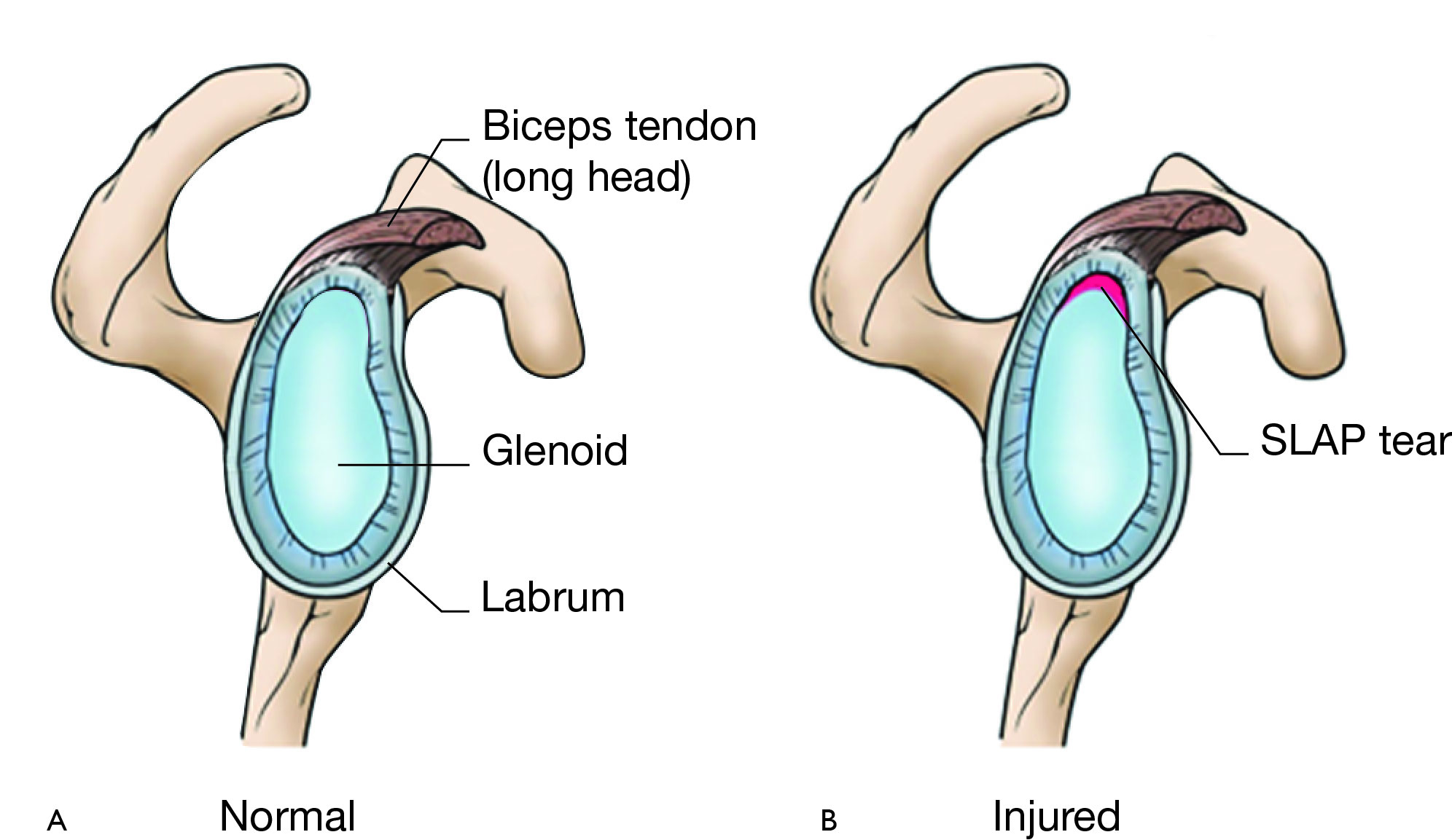
A Superior Labrum Anterior to Posterior tear, called a SLAP tear, is the most common. The name describes the location and direction of the injury – at the top of the labrum, extending from front to back.
SLAP tears are commonly seen in athletes or active individuals who engage in repetitive overhead activities e.g. throwing athletes.
Atraumatic SLAP tears (ones that occur without a specific injury or trauma) are thought to occur due to the significant shear and rotational forces that the biceps tendon must resist, which is thought to “peel back” the labrum.
Traumatic SLAP tears can occur from falling on an outstretched arm or experiencing a sudden pulling force to the arm e.g. grabbing an overhead object to stop a fall, forceful pull of a tow rope when water skiing.
Bankart lesion
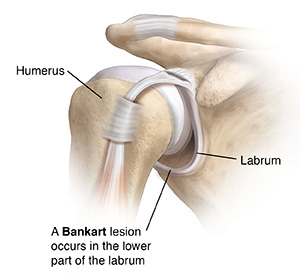
A Bankart lesion is a tear to the labrum that occurs at the bottom of the shoulder socket. This type of tear is typically associated with an instability event such as a dislocation or partial dislocation (subluxation).
— Learn more about shoulder instability here —
Bankart lesions can increase the risk of recurrent shoulder instability due to the disruption of the stabilizing rim (along with other factors such as the size of the tear, the persons overall health, and the integrity of the other structures in the shoulder).
Posterior labral tear
This type of tear occurs at the back of the shoulder and is categorized depending on whether the tear occurred with trauma (e.g. the shoulder travels backwards from a posterior instability event), or without trauma (e.g. from degeneration of the outer edges of the labrum).
Degenerative tears can more accurately be described as fraying along the outer edges from injury or wear and tear. These types of posterior tears rarely cause symptoms and are often considered as part of the normal aging process. In throwing athletes, however, these types of tears can be more pronounced, even at younger ages.
Signs & Symptoms
Despite the differences mentioned above, these injuries share many overlapping signs and symptoms that can include:
- Decreased range of motion
- Loss of strength, especially with lifting
- Popping, catching, grinding sensations
- Shoulder instability
- Shoulder pain, especially with overhead activities
- Loss of throwing speed or “dead arm” sensation
Diagnosis
The diagnostic process begins with an examination by an experienced healthcare practitioner or physician, who will take a detailed history of the injury and identify any risk factors (such as physical demands of work or sport, or previous injuries) that may contribute to it.
Next, both shoulders, along with the cervical spine, will be examined. Due to the depth of the structures involved and the wide range of areas where the injury can occur, it is important to note that the physical exam is not definitive. However, when combined with a detailed history, the exam can provide valuable information to guide initial treatment options.
A sports medicine physician or orthopedic surgeon may suggest an injection of lidocaine without corticosteroids (cortisone) into the shoulder joint for diagnostic clarity. If pain and function improve while the joint is “frozen” by the anesthetic, an injury within the joint can be inferred. On the other hand, if numbing the inside of the shoulder provides no benefit, the source of pain may lie outside the joint.
For some older individuals, a mixture of lidocaine and cortisone can be considered for therapeutic purposes as well. The rationale is that the anti-inflammatory steroid can reduce pain, allowing for more focused strengthening and rehabilitation/physiotherapy.
The best available test for labral tears is magnetic resonance imaging (MRI), which has an accuracy of about 80%. MRI can be enhanced with a stronger machine (higher Tesla strength) or by adding an arthrogram (MRA), which uses dye as a contrast agent to highlight any leakage within the shoulder joint that may indicate a tear. The most accurate diagnosis, however, can only be made through arthroscopy, which involves introducing a camera into the joint. This is an operative procedure that carries inherent risks and benefits.
Treatment
Non-surgical
The mainstay of non-surgical treatment is rest, avoidance of aggravating activities, and strengthening of the rotator cuff to help stabilize the shoulder joint.
In most cases, this type of management can be effective. Research shows that sticking to a proper rehabilitation protocol, can result in success rates as high as 78%.
If pain is stopping a person from carrying out exercise and strengthening, then anti-inflammatory medications or a cortisone injection may be recommended to help facilitate rehabilitation.
While proper rehabilitation is best carried out with the guidance of an expert (physiotherapist/athletic therapist) who can assess and individualize care, here are a few resources that can help start the process:
Surgical
Surgical treatment may be recommended in the case that non-surgical treatment fails, or for certain types of tears e.g. Bankart lesions, or those tears that may lead to shoulder instability.
The type of surgery will depend on several factors that include:
- the type of tear
- sport/occupation/activities
- previous injuries
- shoulder anatomy
Your orthopaedic surgeon will discuss the different approaches and methods to determine the best fit for you and the demands of your activities.
Regardless of treatment, strengthening the shoulder is crucial for a positive long-term outcome.
Expert Contributor

Benson Cho, Certified Athletic Therapist, Vidar Sport Medicine





