
Impingement: a common cause of hip pain
Have you ever experienced pain in the front of your hip or groin?
In his latest Bow Valley Crag & Canyon article, Banff Sport Medicine Physician, Dr. Andy Reed, discusses the potential cause.
Lately it seems that we see a lot of hip injuries in young athletes.
I have even had a handful of younger patients require hip replacements in their late 30s or 40s over the last few years. Whilst hip joint replacement surgery at such a young age is certainly not a common scenario, it’s very unfortunate for the affected individual.
In the early 2000s a condition called Femoroacetabular Impingement (FAI) was first described in detail, and it was suggested that many of these worn out and relatively young hips were affected by the condition.
The link between osteoarthritis of the hip and FAI is no longer in doubt, but fortunately it appears that if picked up early, treatment of FAI may not only alleviate symptoms, but may also prevent the future development of hip osteoarthritis.
What is Femorocetabular Impingement (FAI)?
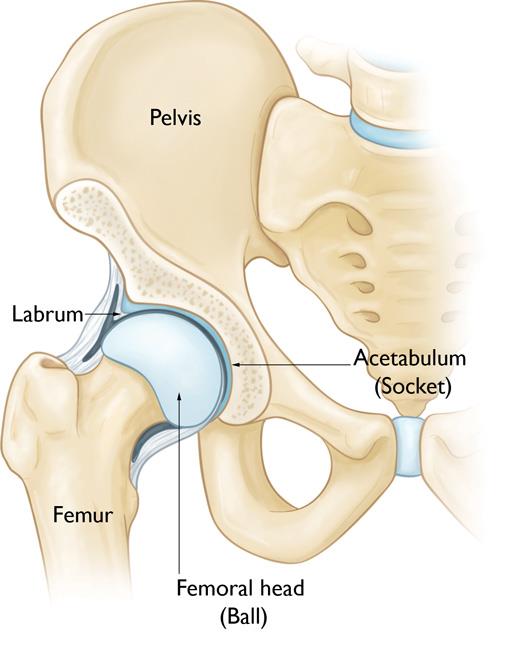
In a healthy hip, the femoral head fits perfectly into the acetabulum.
In FAI, however, there is essentially a mismatch between the shape of ball of the femur and the shape of the socket of the hip.
There are three main types of FAI
Cam Type FAI
In the type that affects males more commonly – called cam type FAI – the shape of the femoral head is more oval than round.
When the hip is flexed this mismatch causes the femur to bump up against the front of the hip socket, eventually causing damage to a structure called the labrum and the cartilage lining the joint. The labrum is a rim of specialized fibrocartilage that acts like a suction cup to stabilise the femur in its socket. It’s a bit like the meniscus in the knee. If it is damaged, the hip joint may become unstable leading to premature wear.
Pincer Type FAI
In another type of FAI the hip socket is the problem; it is excessively deep and therefore covers more of the femur – we call this pincer type FAI. This type of FAI is commoner in females, and can also lead to labral tearing, but it is not so strongly associated with arthritis of the hip.
Combined
Combined FAI is when both cam and pincer coexist in the same joint.
Who is most at risk of FAI?

The typical patient we see with FAI is usually under 40, and very active in sports.
They complain of pain in the front of the hip or groin, which is the usual location for hip joint related pain.
The pain is often described as a deep ache, with a sharper component with extreme hip flexion activities such as squatting. Prolonged sitting can be painful and the hip may feel stiff or restricted. Rotation can be painful, so getting in and out a vehicle may become difficult due to pain. Pain will often be aggravated during sports that require cutting or rapid changes in direction. Running itself can be painful.
The patient may experience a catching sensation in the hip, especially with a labral tear. Labral tears can also cause clicking and clunking in the hip. Sometimes the pain radiates to the outside of the hip or down towards the knee. The patient may recall a specific incident when they slipped and hurt the hip, bit more commonly the onset is gradual.
How is FAI diagnosed?
After an examination in clinic, we will evaluate the hip with x-rays and often an MR arthrogram – an MRI scan with dye injected into the hip joint before the scan.
X-rays will show us if there are obvious bony changes, either cam or pincer type changes, and whether the hip is already showing signs of arthritis.
The MR arthrogram can determine if there is a labral tear, and can show changes in the articular cartilage that may not yet be evident on x-rays.
How is FAI treated?
If FAI is confirmed on imaging, we will sometimes perform an injection of local anesthetic into the hip joint to confirm that the pain originates there.
We will usually refer patients to a physiotherapist to address any weak or tight structures about the hip, which in many cases is effective at improving symptoms.
Depending on the severity of the hip joint changes, referral to an orthopaedic surgeon may be arranged.
Hip arthroscopy with repair or reconstruction of any labral damage can be performed, and the surgeon will address any bony changes around the hip. The femoral head can be contoured with a shaver to restore a normal spherical shape. Without this, any labral repair will ultimately fail.
Bony anatomical changes on the socket side are more complex to correct but can be addressed with procedures such as the peri-acetabular osteotomy.
Ultimately the goal is to restore normal hip anatomy and function, so that not only symptoms resolve, but, more importantly in the long term, to preserve the hip joint such that osteoarthritis does not develop.
Unfortunately, if the joint is already showing significant wear, surgery is far less successful, and in many cases hip preservation surgery will not be recommended.
Patients with arthritis in their hips can be helped to manage their symptoms until a replacement is recommended, so it is important that we see patients with hip pain and FAI before they develop severe cartilage damage.
In my next column I will talk about hip osteoarthritis in more detail.
Expert Contributor

Dr. Andy Reed, Sports Medicine Physician and ultramarathon running M.D.





