Ankle Fractures 101: The Basics
Ankle fractures are usually the result of a harsh rotational force. For example, if you over-roll your ankle in a trip or fall.
A person with an ankle fracture will not tolerate weightbearing activities, so until treated, this injury will prevent a person from standing on the injured foot or walking.
The Ankle Joint
The ankle acts as a rotary-hinge joint. This means we can move our ankle in a circle, point our feet up and down, and move it side to side. This range of movement means a lot of joint mobility, but also makes the joint vulnerable to instability and injury.
The three bones of the ankle joint are the tibia, fibula, and talus. The two main boney bumps of our ankle are the end points of tibia and fibula, called the medial and lateral malleoli (respectively). The third malleolus is the posterior malleolus, the rear bump of the tibia.
The talus bone of the foot sits right below both the tibia and fibula, making the tibiotalar joint —the main ankle joint. The space between the tibia and fibula is called the sesamoid joint.
Normally, the ankle ligaments and malleoli keep the foot within a normal range of motion. Most ankle fractures result from a force that pushes the foot beyond the limits of normal, breaking bone.
As many as 75% of ankle fractures are a result of an outward rotation (i.e., rolling your ankle), usually fracturing the lateral malleolus.
Fractures can also occur more easily when there is already damage to the ligaments and tendons. Certain conditions, such as osteopenia or osteoporosis can also increase the risk of an ankle fracture.
— Read more about osteopenia and osteoporosis here —
Symptoms

Symptoms of an ankle fracture may include:
- Pain
- Swelling
- Bruising
- Damage to blood flow or nerves (numbness, tingling, blueish skin, loss of feeling)
- Deformity
- Inability to weight bear for 4 steps, at the time of injury and when seeking medical care
Diagnosis
When you are assessed by a doctor, they will check your injury for neurovascular status (blood flow, movement and feeling). Any loss of blood flow will need emergency treatment. If your physician suspects an ankle fracture, they will order an x-ray. They may also order a CT scan or MRI, which can assist them complete a more detailed assessment of the joint surfaces, fracture profile, and ligament involvement.
There are many methods a doctor can use to categorize an ankle fracture. Listed below are two methods: one based on which bones are fractured; and the other that lists fractures as stable vs. unstable. This is useful in choosing a treatment method.
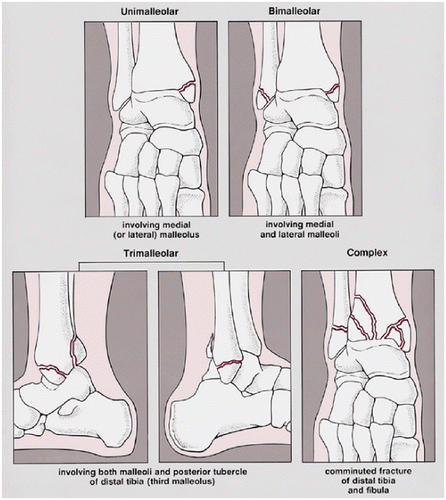
Bone involvement can include:
- Isolated malleolar fracture (unimalleolar): one fracture, usually in the outside ankle bone (lateral malleolus), but can also occur on the inside (posterior), although these are less common
- Bimalleolar fracture: both the inside and outside ankle bone (medial and lateral malleolus)
- Trimalleolar fracture – all three malleoli (lateral, medial, posterior)
- Complex fracture – multiple fractures, with movement of bone fragments
These fractures can then be classified as stable or unstable.
Stable
A single lateral or posterior malleolar fracture, with no bone movement on x-ray while the patient is weight bearing (standing). This means, while there is a fracture, the bone did not split or shift, and healing will likely occur without the need for surgery.
Unstable
Unstable fractures can include:
- Bi- and tri- malleolar fractures
- Complex fractures
- Fracture plus joint dislocation
- Single lateral malleolar fracture, with a widening of the ankle joint space >5mm on x-ray while patient is weight bearing
Treatment
The goals of treatment are to restore joint alignment, stability, and reduce the risk of post-injury arthritis.
Ankle fractures can be treated either with or without surgery.
Stable fractures may be treated non-operatively. A brace, cast or air boot will be used to protect the ankle while the fracture heals. You doctor will order x-rays in the first 2-3 weeks post injury to ensure the fracture is healing in proper alignment.
Unstable fractures are usually treated operatively, and will included internal hardware (surgical plates, wires, screws, etc.) to correct the fracture. Most commonly the procedure will be an open reduction with internal fixation (ORIF), meaning the surgeon will make an incision to access the injury site and use hardware to correct it.
Both treatment options include joint immobilization in the first stages of healing, which is done with a brace or a removeable boot. This may include 6-8 weeks of non-weight bearing, depending on the fracture.
Once weightbearing is allowed, a gradual return to exercise and a physiotherapy program (in particular, recovery from unstable injuries) will help to improve joint function and stability. In general, full weightbearing and participation in work and recreational sports can be reached within 12-16 weeks post-injury(8). Actual recovery times will vary among patients and injury specifics.
Outcomes
Recovery from a stable ankle fracture that is treated non-surgically is excellent, with an anticipated full return to pre-injury activities and sports as early as 6-8 weeks.
In the case of unstable fractures requiring surgery, however, ankles will take longer to regain range of motion, from 1 to 2 years. Some people may find that they can’t move their ankle as much as they could before their injury, and there is a 10% risk of developing arthritis long-term.
Contributing Expert
Bree Kullman, University of Calgary, Doctor Of Medicine, Class of 2024, ACMG Hiking Guide & Climbing Instructor
References
Goost, Hans, et al. “Fractures of the Ankle Joint.” Deutsches Ärzteblatt International, vol. 111, 23 May 2014. https://www.aerzteblatt.de/, www.aerzteblatt.de/int/archive/article/160219, 10.3238/arztebl.2014.0377. Accessed 27 Mar. 2022.
Hong, C. C., Roy, S. P., Nashi, N., & Tan, K. J. (2013). Functional Outcome and Limitation of Sporting Activities After Bimalleolar and Trimalleolar Ankle Fractures. Foot & Ankle International, 34(6), 805–810. https://doi.org/10.1177/1071100712472490
Moseley, A. M., Beckenkamp, P. R., Haas, M., Herbert, R. D., Lin, C. W., & EXACT Team (2015). Rehabilitation After Immobilization for Ankle Fracture: The EXACT Randomized Clinical Trial. JAMA, 314(13), 1376–1385. https://doi org.ezproxy.lib.ucalgary.ca/10.1001/ jama.2015.12180
Pakarinen H. Stability-based classification for ankle fracture management and the syndesmosis injury in ankle fractures due to a supination external rotation mechanism of injury. Acta Orthop Suppl. 2012 Dec;83(347):1-26. doi: 10.3109/17453674.2012.745657. PMID:23205893.
Tartaglione, J. P., Rosenbaum, A. J., Abousayed, M., & DiPreta, J. A. (2015). Classifications in Brief: Lauge-Hansen Classification of Ankle Fractures. Clinical orthopaedics and related research, 473(10), 3323–3328. https://doi.org/10.1007/s11999-015-4306-x
Warner, Stephen J. MD, PhD*; Garner, Matthew R. MD*; Hinds, Richard M. MD*; Helfet, David L. MD†; Lorich, Dean G. MD† Correlation Between the Lauge-Hansen Classification and Ligament Injuries in Ankle Fractures, Journal of Orthopaedic Trauma: December 2015 – Volume 29 – Issue 12 – p 574-578 doi: 10.1097/BOT.00000000000003 93
Wire J, Hermena S, Slane VH. Ankle Fractures. [Updated 2021 Aug 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from:https://www-ncbi-nlm-nih-gov.ezproxy.lib.ucalgary.ca /books/NBK542324/