
Return to sport and activity after MPFL reconstruction
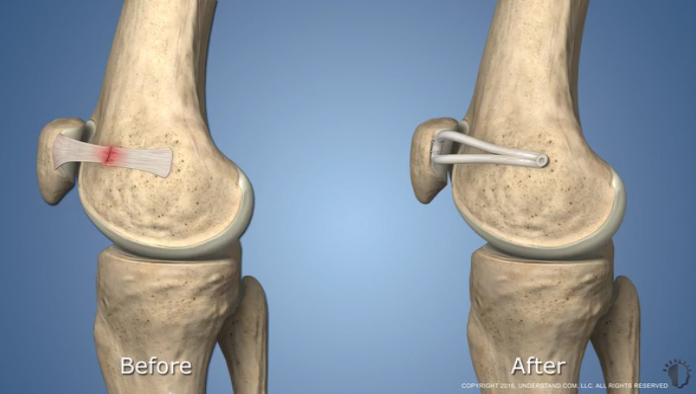
A medial patellofemoral ligament (MPFL) reconstruction, MPFL-R, involves replacing the damaged ligament with a tissue graft, either from a person’s own tissue or from a donor.
The MPFL is the main ligament that stabilizes the kneecap (patella) and prevents it from dislocating to the outside (lateral) of the knee.
It is often damaged when the kneecap dislocates and moves out of its normal position – the groove at the end of the femur (thigh bone). These dislocations can occur from injuries during sports, such as a direct impact to the knee, or from variations in a person’s anatomy (trochlear dysplasia, patella alta, generalized joint laxity, etc.).
While injury to the MPFL can be treated without surgery, surgery may be necessary in cases of severe ligament tears, recurrent patellar dislocations, and in patients with high-risk anatomy.
Learn more about the basics of MPFL reconstruction
Recent studies have shown that MPFL reconstruction is an effective treatment, with 92.8% of patients returning to sport and 71.3% returning at the same or higher level of play (Platt et al., 2021). Of those who did not return to sport, the main reasons were fear of reinjury, loss of knee function, loss of interest, or lack of time.
While the initial stages of healing and strengthening following MPFL reconstruction may only take between 9 to 18 weeks, the expected time before most patients return to a full level of play is closer to 2 years.
However, this time to return to sport depends on many factors and can be slightly reduced with strong dedication to the rehabilitation protocol.
The timeline for returning to sport
The timeline for returning to sport depends on how well a patient moves through a phased rehabilitation program.
Progression through each phase is not based on time restrictions but on a healthcare professional’s assessment of the individual’s rehabilitation stage – with commitment to the program and to all recommendations being vital for a successful recovery.
In phase 1, the early postoperative phase (usually the first 1-3 weeks after surgery), the main goals are knee bracing to protect the graft, using cold therapy and elevation to control pain and swelling, and beginning gentle exercises for quadricep (thigh) strengthening.
Phases 2 and 3 are the initial and progressive strengthening phases, with a focus on quadriceps, hamstring, hip, and core strength. During phase 2, typically 3-12 weeks after surgery, the patient transitions from a hinged knee brace to a patella stabilizing brace and begins to wean off crutches. While phase 3 usually lasts 9-18 weeks, it can take up to 6 months to fully master. During this phase, the intensity of strengthening is increased, and patients must show improved endurance and a full range of motion before moving to phase four.
Finally, phase 4 is the sport readiness phase and focuses on agility during dynamic exercises (e.g., jumping, hopping, running) and a return to sport-specific motions and drills. For example, a soccer player would return to dribbling the soccer ball and practicing shooting drills. This phase typically begins 18 weeks into recovery and may last up to 2 years.
This “sport readiness” phase can also be considered on a continuum, or something that progresses over time.
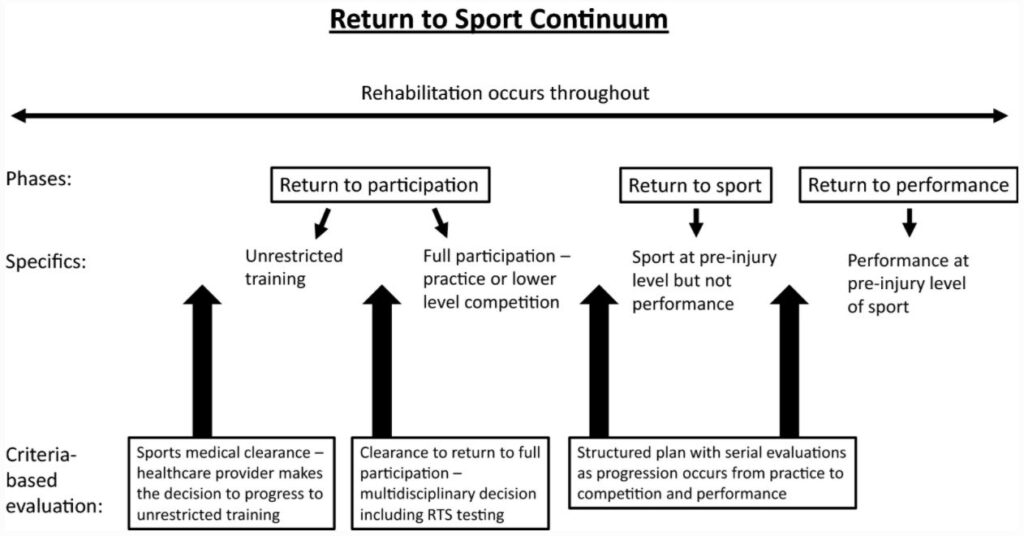
During the phase of return to participation, the patient is physically active, may train, but is medically, physically and/or psychologically not yet ready to return to sport.
During the return to sport phase, the patient has returned to their defined sport, but the desired performance level hasn’t been reached.
During the return to performance phase, the patient has returned to their defined sport and performs at their pre-injury level.
See the full Banff Sport Medicine post-operative MPFL rehabilitation program
The decision to return to sport
The final decision about whether a patient is ready to return to sport is made collaboratively between the surgeon, the physiotherapist, the patient, and the patient’s coach. The main factors considered are quadriceps, hip and core strength, and the ability to perform sport-specific activities safely.
However, other factors are also considered, including:
- Graft healing: The MPFL graft should be well healed by the time quadricep strength and control are mastered.
- Neuromuscular control: This is the unconscious but trained coordination between the nerves and the muscles that helps keep joints stable during movement.
- Psychological readiness: Psychological factors are as important as physical factors when determining if a patient is ready to return to sport. Fear of reinjury and kinesiophobia (fear of movement) are major reasons that prevent patients from returning to sports.
- Other knee injuries: other injuries that occur inside the knee at the same time, such as chondral bone injuries, can delay the recovery process and sometimes limit the ability to successfully return to sport (especially at the same level of play).
Many factors influence the decision to return to sports, which can help explain the wide variation in recovery time.
It is important to remember that each patient’s situation is unique, and that the decision to return to sport should be based only on the individual’s timeline and should never be rushed.
8 tips to improve your chances of returning to sport and activity
While phase four of rehabilitation is crucial in re-training sport-specific exercises, it is not the only phase that matters in the process of returning to sport and activity. Studies have shown that adherence to rehab protocols both in the time periods just before surgery and just after surgery are important in laying the foundations of the recovery process.
Below are some tips to ensure a strong foundation that will improve the chances of successfully returning to sport.
Complete a “prehabilitation” program. Regaining strength and movement in the injured limb before surgery helps reduce recovery time and lowers the risks of complications (e.g., deep vein thrombosis). Get the Banff Sport Medicine Prehab Protocol here.
Dedicate time to stick to your rehabilitation program. Setting out time during your day specifically for rehab exercise can help you adhere to the rehab protocol. Sticking to and completing your protocol is one of the most important aspects to enable a return to sport.
Use your brace properly. Bracing after surgery protects the knee while the quadricep muscles are weak. It is important that the brace is used until enough strength and function are restored to prevent reinjury.
Don’t neglect range of motion exercises. The prescribed range-of-motion exercises will not stretch the MPFL graft and are important to recovery. Make sure that range of motion requirements are met before proceeding to the next phase of rehabilitation.
Use electrical muscle stimulation (EMS). EMS helps regain strength safely and will not harm the MPFL graft. It is recommended to combine EMS with voluntary muscle contraction at all phases of recovery.

Use cold therapy. Cold therapy and icing are vital to controlling pain, inflammation and swelling after surgery. Research has shown that cold therapy can decrease the need for pain medication following surgery. Learn more about cold therapy here.
Avoid straining the MPFL graft. A valgus knee (knock knee) position can strain the MPFL graft and should be avoided. Strengthening the quadriceps and hips while being aware of knee alignment is crucial to prevent this strain. This is especially important during dynamic movements (e.g., jumping and running) and landings.
Don’t compare your recovery to others! Remember that not everyone’s recovery will look the same and that you should only return to sport on your timeline. Your sport of choice, level of play, age, source of injury, and desire to return to sport all play a role in the timeline to recovery.
References
Garvey, K. D., Lowenstein, N. A., & Matzkin, E. G. (2022). Anterior Cruciate Ligament Injury Prevention. In The Female Athlete (pp. 49-63). Elsevier.
Li, Z. I., Triana, J., Lott, A., Rao, N., Jazrawi, T., Montgomery Jr, S. R., … & Campbell, K. A. (2023). Patients who undergo bilateral medial patellofemoral ligament reconstruction return to sport at a similar rate as those that undergo unilateral reconstruction. Knee Surgery, Sports Traumatology, Arthroscopy, 31(10), 4195-4203.
Meredith SJ, Rauer T, Chmielewski TL, et al. Return to sport after anterior cruciate ligament injury: Panther Symposium ACL Injury Return to Sport Consensus Group. Knee Surg Sports Traumatol Arthrosc. 2020;28(8):2403-2414.
Niemuth, E., & Monson, J. (2020). Surgical Rehabilitation for Select Patellar Stabilizing Procedures. Patellofemoral Pain, Instability, and Arthritis: Clinical Presentation, Imaging, and Treatment, 359-378.
Platt, B. N., Bowers, L. C., Magnuson, J. A., Marx, S. M., Liu, J. N., Farr, J., & Stone, A. V. (2022). Return to sport after medial patellofemoral ligament reconstruction: a systematic review and meta-analysis. The American Journal of Sports Medicine, 50(1), 282-291.





