
Hip Impingement: Evidence Based Treatment Options
You have been diagnosed with femoroacetabular impingement (FAI), more commonly known as hip impingement, and you may be thinking “Well, now what?”
FAI is a condition where physical abnormalities cause the bones of the hip joint to rub together during movement. This abnormal movement, or “impingement”, can damage the soft tissues within the hip joint, leading to pain, stiffness, and other symptoms.
— Learn more about the basics of hip impingement —
Hip impingement can be caused by either a pincer deformity, a cam lesion, or in some cases both.

Treatment options for hip impingement
Treatment options for hip impingement include both non-operative and operative, with the best option dependent on many factors, including what is causing your impingement.
Non-operative treatment options
Non-operative management is typically considered the first-line treatment for patients with mild to moderate symptoms. This option often includes a period of rest, activity modification, physiotherapy, and injections.
Rest and activity modification
If you are experiencing pain and discomfort in your hip, an initial period of rest from activity can be beneficial. Once your symptoms settle, it is important to avoid activities and positions that worsen your pain. Activities that require repeated rotation of the hip (ex. golf, baseball and ballet) or those that require deep flexion (squatting) or adduction (ex. yoga, hockey goaltending) have been shown to increase the friction in the bones of the hip and worsen hip pain.
Physiotherapy
Many patients with hip impingement who are treated with physiotherapy and activity modification can experience significant improvement in symptoms.
For successful outcomes, understanding the implications of the physical deformity on range of motion and muscle activation is important, as are specific exercises tailored to each individual.
There are a variety of different physiotherapy programs available online. Here is just one example.
Programs should:
- Not include hip range of motion as a treatment goal. Patients with hip impingement can be quite stiff. Many physiotherapy programs will try to work on improving mobility. However, for patients with FAI they should avoid positions which cause impingement (extremes of hip flexion, abduction and internal rotation) as these positions can make their pain worse.
- Include core strengthening and stability. Programs with an active focus on building core muscle strength and stability have been shown to be more affective at improving symptoms than routines without this. This involves strengthening the muscles in the abdomen and the back.
- Include muscle strengthening. Along with core strengthening, programs should also focus on strengthening the quadriceps, hamstrings, gluteal muscles and other muscles surrounding the hip joint.
- Aim to correct movement impairments and poor postural habits. Correcting movement impairments and postural habits should be done within the limits of pain. Poor posture and mechanics can lead to increased compressive loads in the hip and lead to imbalance of the surrounding muscles.
Medications
Non-steroidal anti-inflammatory drugs (NSAID’s) such as ibuprofen can help reduce pain and discomfort caused by hip impingement. These are available either over the counter or in prescription strength forms.
— Learn more about the basics of NSAIDs here —
Injections
Hip injections are commonly performed under ultrasound guidance or with the use of X-ray.
These injections can be used to help diagnose hip impingement or to treat it. Injection options include local anesthetic (freezing), corticosteroids and hyaluronic acid.
Diagnostic Injections: Some patients with hip impingement may have other causes of pain around the hip. Studies have shown that pain relief from intra-articular injections can help support the diagnosis of FAI. Furthermore, patients who experience pain relief from injection of local anesthetic are more likely to benefit from surgical management.
Therapeutic Injections: Some patients may get up to 12 months of symptom relief from intra-articular injections. Hyaluronic acid was found to be the most effective at providing pain relief with significant improvements in outcome measures. Corticosteroids may provide some symptom relief, but studies show it may not be as effective. Therapeutic injections are particularly useful in patients with underlying arthritis or in those who are not surgical candidates.
Operative treatment options
Operative management is recommended for patients with more advanced symptoms and underlying physical causes.
This treatment option focuses on correcting the abnormality that is causing the impingement – either a pincer deformity, a cam lesion, or in some cases both.
Studies have shown that for many patients, particularly younger patients, surgery can help improve symptoms and allow patients to return to full activities. It can also be helpful to prevent the development of early osteoarthritis by restoring normal anatomy. Older patients, or those with more advanced osteoarthritis, may be candidates for a total joint replacement.

Surgical management may include the following:
Repairing or reconstruction the torn labrum
The labrum (ring of cartilage that surrounds the hip socket) can get damaged due to hip impingement.
In most cases, damage to the labrum is cleaned out (debrided) or repaired using special anchors and suture. However, in some cases the labrum is not able to be repaired and some surgeons will perform a reconstruction which involves creating a new labrum with a tendon from the patient or a tissue donor. Early research suggests that repair of the labrum provides a better anatomic result and improved outcomes when compared with debridement.
Resection of bony deformity
In patients with a pincer deformity, the extra bone around the acetabulum is carefully shaved away. This is called a pincer resection aka “acetabular osteochondroplasty”.
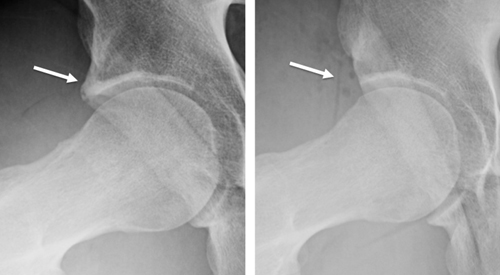
In patients with a cam deformity, this is carefully shaved away to restore the normal “ball-shape” of the head of the femur. This is called a cam resection aka “femoral osteochondroplasty”.

Reproduced from Diaz-Ledezma C, Higuera CA, Parvizi J: Mini-open approach for the treatment of FAI in Sierra RJ, ed: Femoroacetabular Impingement. Rosemont, IL, American Acad of Orthopaedic Surgeons, 2013, pp 81-91.
Surgical techniques
The available surgical options can be categorized broadly as open surgical dislocation or arthroscopy (hip scope). This is usually based on surgeon preference or the deformity present. Some patients with other underlying deformities may require larger surgeries which will not be covered in this article.
Open Surgical Dislocation: Open surgical dislocation involves a large incision and used to be the gold standard for treatment of hip impingement. However, with advances in arthroscopic techniques, arthroscopy has become more common. Some patients with larger deformities or other underlying conditions (ex. Perthes disease) may not be candidates for arthroscopy.
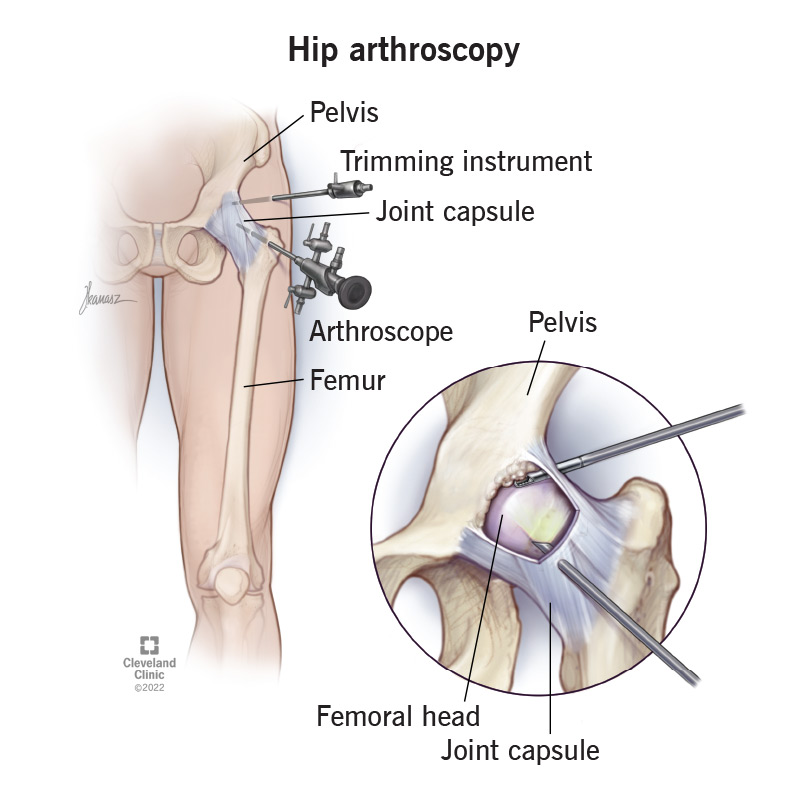
Hip Arthroscopy: Hip arthroscopy is a minimally invasive technique which involves 2-3 poke-hole incisions and the use of a camera to perform the procedure. Recent literature shows outcomes of hip arthroscopy are equivalent to open surgical dislocation with decreased complications and allows for quicker return to activity.
Contributing Expert
Christopher Hewison MSc, MD, FRCSC, Clinical Fellow in Orthopaedic Sports Medicine




