
Chronic Exertional Compartment Syndrome
~ A Pain in the Compartment ~
Chronic exertional compartment syndrome (CECS) is an exercise-induced condition that commonly affects the muscles and nerves of endurance athletes.
It is seen most often in athletes under the age of 30 who train in a repetitive impact activity, such as running.
The syndrome causes a set of symptoms that occur after a predictable amount of exercise, for example, the onset of pain and burning occurring 15 minutes into a run[1].
Both non-operative and operative management options are available.
The Basics
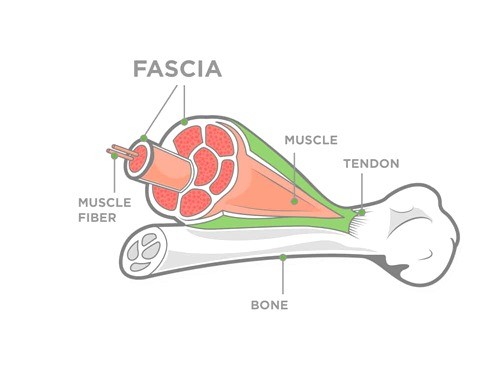
Your limbs are divided into groupings called compartments by a type of tissue called fascia. This separates muscles, nerves, and blood vessels into well-defined regions and holds them in place.
During exercise, muscles expand and produce waste products such as lactic acid.
Compartment syndrome occurs when the local metabolism cannot clear these byproducts fast enough. As waste products and fluid builds up, so does pressure, and the fascia cannot expand enough to accommodate this change.
This increased pressure causes decreased blood flow to the muscles and nerves of the compartment, which results in the symptoms of CECS.
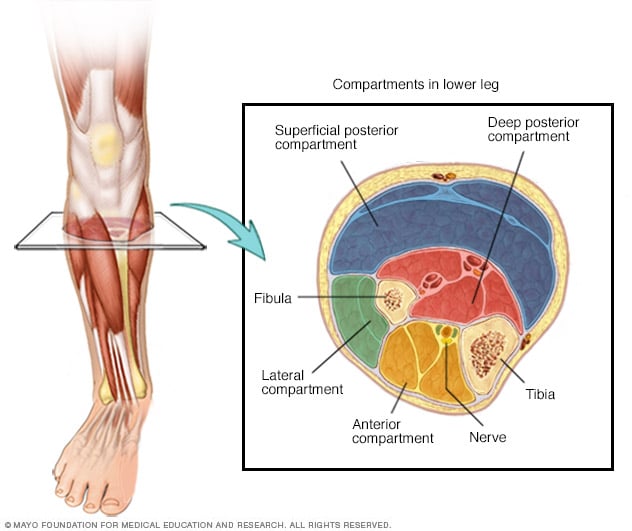
Different limbs have a different number of fascial compartments. The upper arm is divided into two, the thigh into three, and the lower limb into four.
The most commonly affected compartment in CECS is the anterior (front) of the shin[2]. This compartment contains the tibialis anterior, extensor digitorum longus, extensor hallucis longus, and fibularis tertius muscles, along with the anterior tibial artery and deep peroneal nerve. Collectively, these structures act to pull your foot up towards your shin (or dorsiflex your ankle) and to pull your foot up and in (or invert your ankle).
Symptoms
Symptoms of CECS typically occur for athletes at a specific level of exercise and are relieved by rest. This level is variable for each person, but athletes will recognize a certain duration, distance, or intensity of activity that consistently reproduces their symptoms.

Athletes can experience any of the following within the affected compartment of the limb.
- Aching muscles
- Burning pail
- Tightness or cramping
- Numbness and tingling
- Weakness
- Swelling or bulging of muscles
- Severe Foot Drop (difficulty lifting the front of your foot up)
Diagnosis
In order to diagnose CECS, your doctor might suggest investigations that rule out other causes of pain in this region, such as tendonitis and stress fractures. This may involve a physical exam putting pressure along your tibia (shin bone) and tendons of your muscles, and an x-ray or bone scan of the lower limb.
Compartment Pressure Testing is the definitive diagnostic test for CECS[3]. To measure the pressure in a compartment, your doctor will inject a small amount of anesthesia into the affected muscles in order to numb them. A handheld device attached to a needle will be inserted into the compartment, and the pressure will be measured at rest and after a short duration of exercise. If either of the readings is higher than expected, a diagnosis of CECS is made.
Treatment
Treatment of CECS can be both non-operative and operative options. Typically, non-operative treatment for a duration of 6-12 weeks is recommended in the first instance[4].
Non-operative management consists of a number of the following:
- Anti-inflammatory medications, such as Advil or Aleve
- Physiotherapy, stretching, and massage aimed at loosening the fascia
- Activity modifications or cross-training
- Gait assessment to identify and correct movements causing muscle overload
- Orthotics to redistribute weight across the foot
If these conservative, non-operative treatments are not effective in controlling symptoms, your doctor may recommend a surgical procedure called a fasciotomy.
This involves cutting open the tough fascia surrounding the affected compartment, so that the pressure can be relieved.
For anterior leg compartment syndrome, the procedure is often carried out with an incision (cut) on either side of the shin. Recovery from the procedure takes an estimated 12 weeks, starting with no weight-bearing and progressing back step-wise back to activity as tolerated. Approximately 75% of those who undergo an elective fasciotomy return to full function post-operatively.
Contributor
Halli Krzyzaniak, Doctor of Medicine Program, University of Calgary, Cumming School of Medicine.
Citations
[1] Tucker, Alicia K. “Chronic Exertional Compartment Syndrome of the Leg.” Current Reviews in Musculoskeletal Medicine 3.1 (2010): 32-37. Web.
[2] Wuellner, John C., MD, Nathe, Connor, BS, Kreulen, Christopher D., MD, Burnham, Kevin J., MD, and Giza, Eric, MD. “Chronic Exertional Compartment Syndrome: The Athlete’s Claudication.” Operative Techniques in Sports Medicine25.2 (2017): 52-58. Web.
[3] Roscoe, David, Roberts, Andrew J, and Hulse, David. “Intramuscular Compartment Pressure Measurement in Chronic Exertional Compartment Syndrome.” The American Journal of Sports Medicine 43.2 (2015): 392-98. Web.
[4] George, Christopher A., MD, and Hutchinson, Mark R., MD. “Chronic Exertional Compartment Syndrome.” Clinics in Sports Medicine 31.2 (2012): 307-19. Web.





